The Karius Test Can Help You Complete The Fever Of Unknown Origin Puzzle
Diagnostic Application: Fever of Unknown Origin
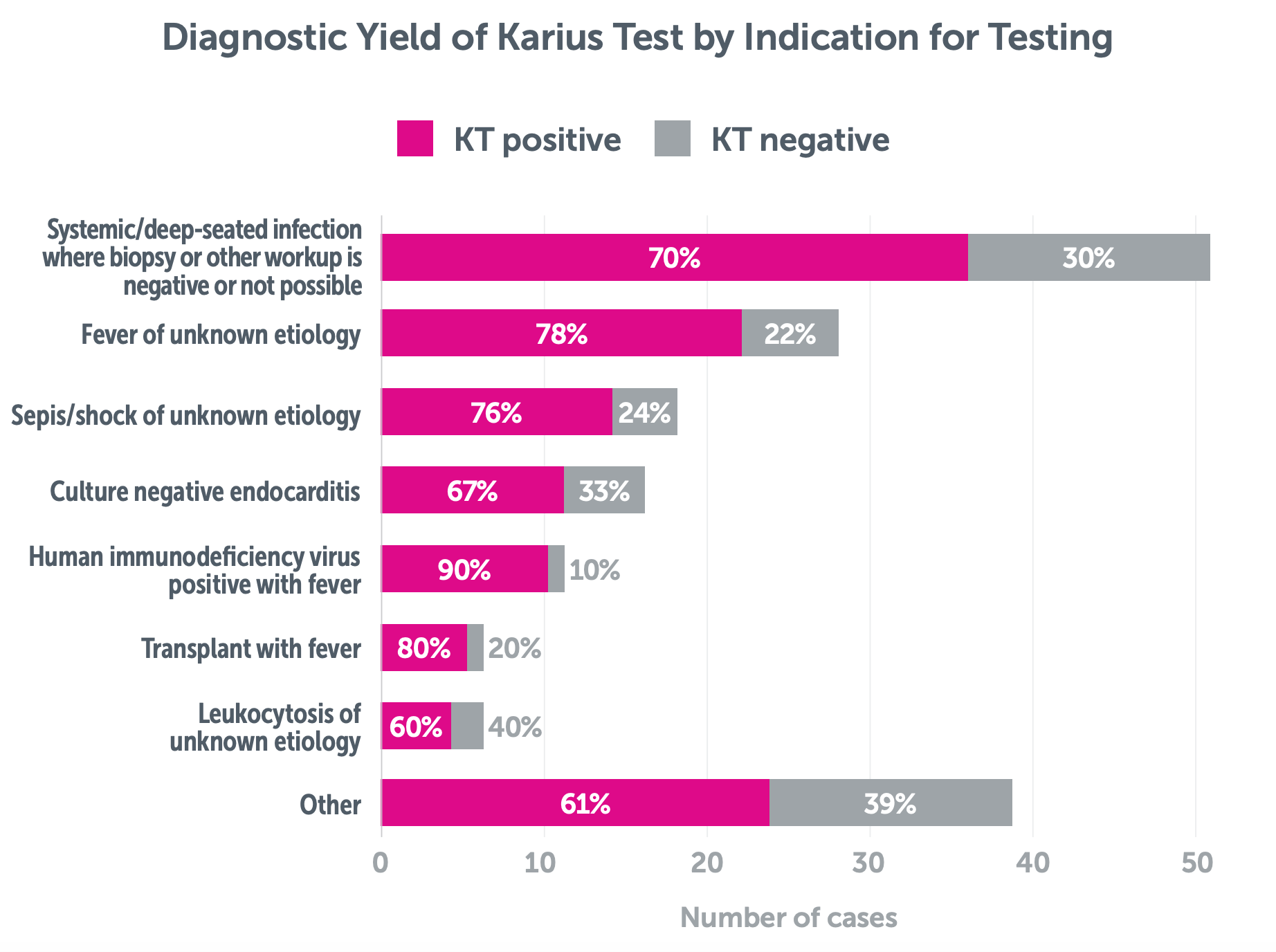
Infections comprise a significant percentage of fever of unknown origin (FUO) cases, accounting for 16%–55% of cases.1,*
Featured Case2
Study Site: Mayo Clinic (Rochester, MN)
A healthy 32-year-old male presented with a 3-week history of FUO and exposure history for recent deer hunting. Exam was notable for left upper quadrant tenderness and scleral icterus. Laboratory evaluation noted elevated liver enzymes, hyperbilirubinemia, lymphopenia, thrombocytopenia, hyponatremia, acute kidney injury, and elevated inflammatory markers.
Tests Performed: Bone marrow biopsy, peripheral flow cytometry, lymph node biopsy, and TTE were negative. Targeted infectious workup was performed, notable for an initial negative Coxiella serum PCR.
Karius Test Result: Coxiella burnetii
Outcome: Initiation of 12-month course of doxycycline and hydroxychloroquine for treatment of acute Q fever complicated by HLH-like syndrome and positive anti-phospholipid antibody.
Clinical Evidence
Study Site: Baylor St. Luke’s Medical Center3,4
In a retrospective study of 167 adult, hospitalized patients, where 55 patients presented with ‘fever of unclear etiology’, use of the Karius Test led to a change in antimicrobial management in 76% (120/167) of cases.

Study Site: Driscoll Children’s Hospital5
In a single-center retrospective study of pediatric patients 21 years old and younger (n=182) where 66% (120/182) of patients had a FUO origin, Karius Test (KT) results had a positive clinical impact** on diagnosis in 32% (59/182) of patients.
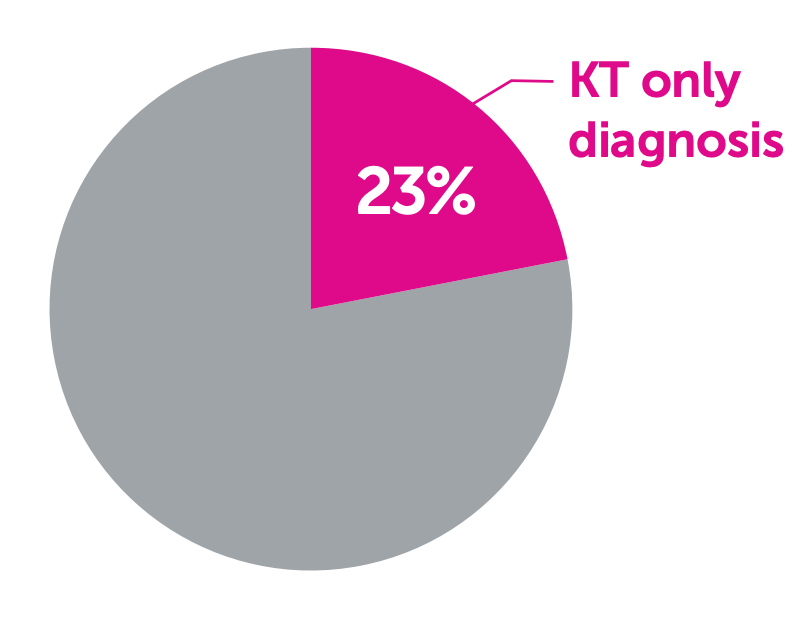
KT was the only diagnostic modality that provided a result in 23% (41/182) cases, including cases of Streptococcus pneumoniae, Pneumocystis jirovecii, Rickettsia typhi, and Bartonella henselae.

*This range was based an analysis of multiple published studies and case series from different locations, including both adult and pediatric hospitalized patients.
**Positive clinical impact was defined as: (1) no change in diagnosis confirmed by KT, (2) new diagnosis confirmed by only KT, or (3) earlier new diagnosis confirmed based on KT result, later confirmed by CT
Considerations for Use

*Distribution of FUO etiologies: infectious 38%, no diagnosis 23%, inflammatory disorders 21%, cancer 12% and miscellaneous conditions 6%.1
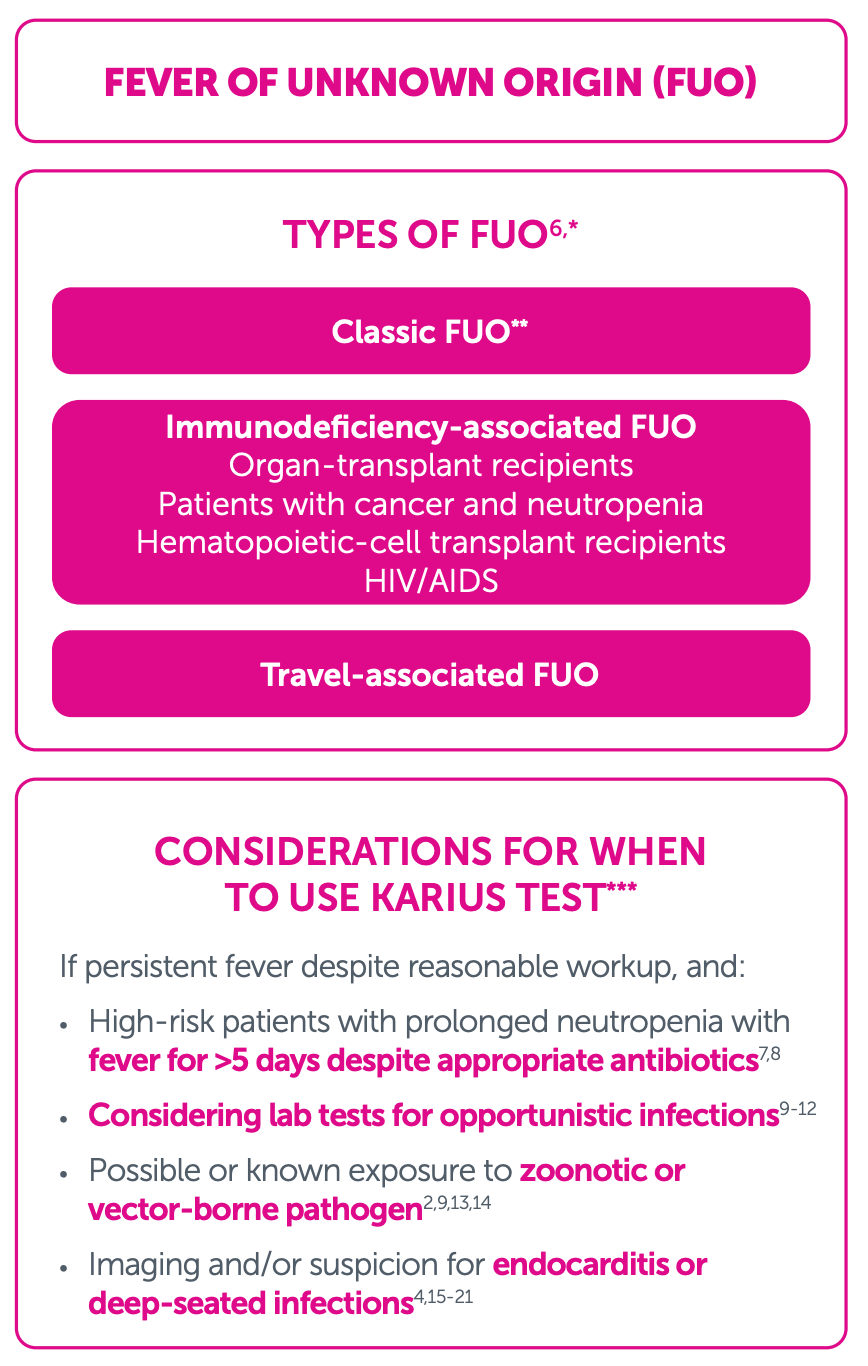
**Classic FUO despite reasonable initial investigations in the inpatient or outpatient setting; includes FUO in persons with HIV infection who are virally suppressed, with CD4 counts >200 cells/mm3; causes fall into four categories: infections (e.g., tuberculosis, endocarditis, occult abscesses, Whipple’s disease, enteric fever, syphilis [mainly secondary], various zoonoses, and histoplasmosis), cancer, autoimmune and autoinflammatory disorders, and miscellaneous causes.
***KT is an LDT. Clinicians should independently evaluate its use and interpret test results. This content is provided for informational purposes only and is not intended or implied to be an exhaustive list of consideration or substitute for existing medical expertise or guideline recommendations. Note that KT has not been studied for negative predictive value.
References:
- Wright WF, et al. Open Forum Infect Dis. 2020 May 2;7(5):ofaa132.
- Ranganath N, et al. Open Forum Infect Dis. 2022 Dec 12;10(1):ofac666.
- Francisco DMA, et al. Poster Presented at: IDWeek Online; Poster# 680; 2020, October 22-25
- Francisco DMA, et al. Antimicrob Steward Health Epidemiol. 2023 Feb 17;3(1):e31
- Li G, et al. Poster presented at: Pediatric Academic Societies
Meeting; Poster #425; 2023, April 27-May 1; Washington, D.C. - Haidar G, Singh N. N Engl J Med. 2022 Feb 3;386(5):463-477.
- Benamu E, et al. Clin Infect Dis. 2022 May 3;74(9):1659-1668.
- Yu J, et al. Transplant Cell Ther. 2021 Jun 15;27(6):500.e1-500.e6.
- Park SY, et al. J Clin Microbiol. 2023 Aug 23;61(8):e0185522.
- Foong KS, et al. Open Forum Infect Dis. 2022 Dec 2;9(12):ofac652.
- Hong DK, et al. Diagn Microbiol Infect Dis. 2018 Nov;92(3):210-213.
- Vissichelli NC, et al. Transpl Infect Dis. 2023 Feb;25(1):e13954.
- Centeno FH, et al. Antimicrob Steward Health Epidemiol. 2024 Feb
12;4(1):e20. - Nguyen-Tran H, et al. Pediatr Infect Dis J. 2024 Jan 18:10.1097/INF.0000000000004255.
- Eichenberger EM, et al. Clin Infect Dis. 2022 Jun 10;74(11):2020-2027.
- Eichenberger EM, et al. Clin Infect Dis. 2023 Feb 8;76(3):e1492-e1500.
- To RK, et al. Pediatr Infect Dis J. 2021 May 1;40(5):486-488.
- Shishido AA, et al. BMC Infect Dis. 2022 Apr 13;22(1):372.
- Solanky D, et al. Front. Trop. Dis. 2022 Mar 24;3:842100.
- Fowler VG, et al. Clin Infect Dis. 2023 Aug 22;77(4):518-526.
- Baddour LM, et al. Circulation. 2015 Oct 13;132(15):1435-1486